In recent years, the laser has gone from a distant promise to a part of the daily routine of otolaryngology (ENT). But there is a common misconception: people talk about “the laser” as if it were a single thing, when in fact there are several types, each behaving differently within the tissue. A laser used to reduce turbinates is not the same as the one used to treat snoring, and neither is the same as the one that cuts and coagulates soft tissue.
In this article, the goal is to explain, in accessible terms, how a laser acts on the body and to present three examples used in ENT: the holmium laser in turbinoplasty, the blue laser in diseases of the larynx and vocal folds, and the Fotona laser in the treatment of snoring and obstructive sleep apnea. The idea is not to say which one is “best,” but to show that each has its own target and purpose.
How a laser acts on tissue: the idea of a target
A laser is, essentially, light of a single wavelength, a single, highly concentrated “color,” even when that light is invisible to our eyes. What makes a laser useful in medicine is the following principle: each wavelength is preferentially absorbed by a different component of the tissue. That light-absorbing component is called a chromophore, and it works as the laser’s “target.”
In practice, two targets matter a great deal in ENT:
- Water, present in almost all soft tissue, absorbs infrared light very well. It is the target of the holmium and erbium lasers.
- Hemoglobin (in blood) and melanin absorb light in the blue and green range. This is what allows the blue laser to act on blood vessels, a property called photoangiolytic.
When the light is absorbed, it turns into localized heat. And depending on the power, the pulse duration, and the mode of application, this heat can produce quite distinct effects:
- Ablation: vaporizing or cutting the tissue.
- Coagulation: sealing small vessels and reducing bleeding.
- Non-ablative thermal effect: simply heating in a controlled way, without cutting or removing tissue, which stimulates collagen.
Add to this the depth that each wavelength reaches: some act more on the surface, others penetrate a little more, and it becomes easier to understand why each laser is chosen for a specific task. This reasoning guides the three examples that follow.
Holmium laser (Ho:YAG) in turbinoplasty
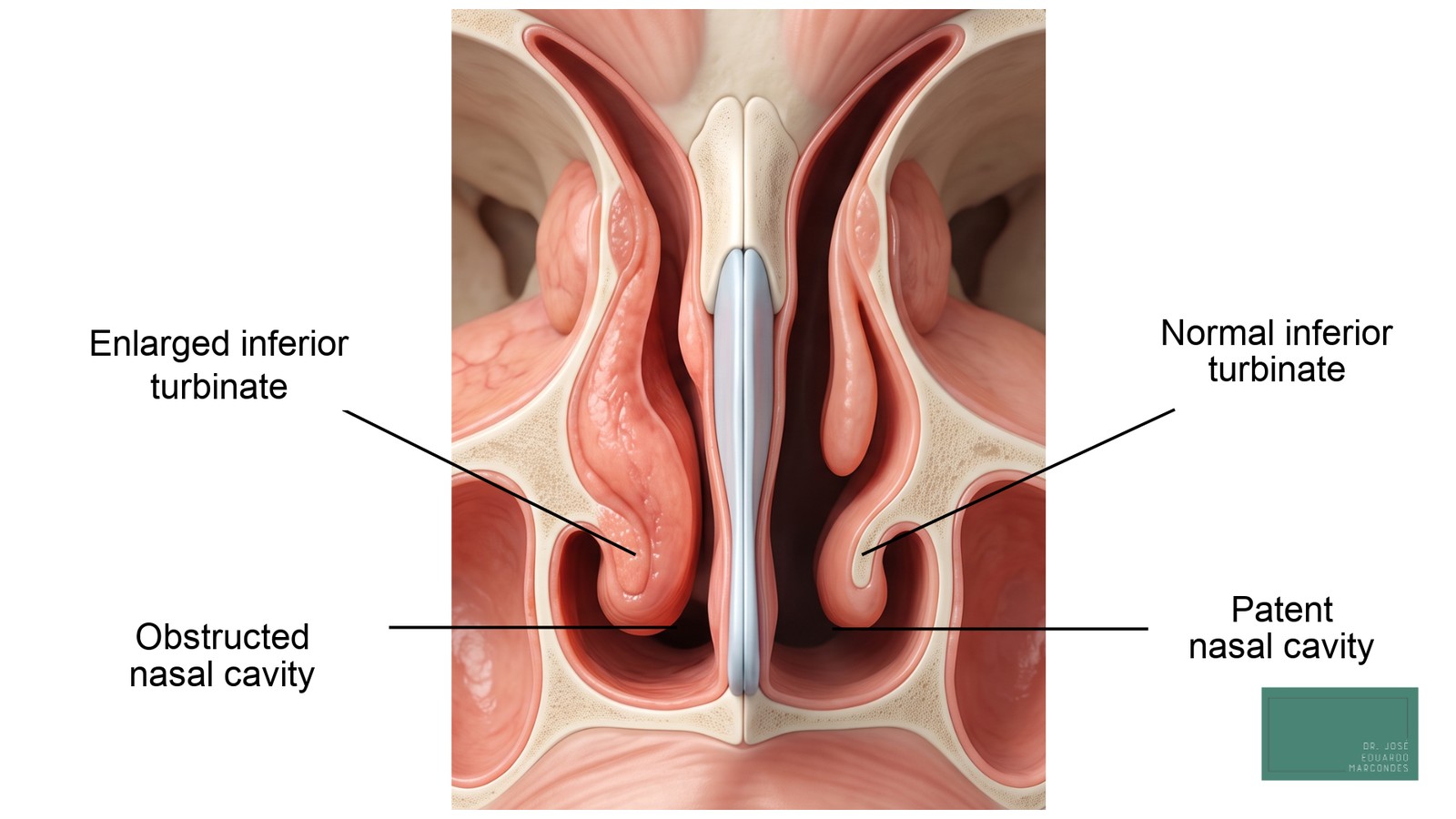
The nasal turbinates are structures inside the nose that warm, humidify, and filter the air we breathe. The problem arises when they swell chronically, something common in rhinitis and allergy, and begin to obstruct the airflow. The result is that feeling of a stuffy nose that does not improve, disrupts sleep, and does not respond to medication alone.
Turbinoplasty is the procedure that reduces the volume of the turbinate to unblock the nose, while taking care to preserve its function. This is where the holmium laser comes in (technical abbreviation Ho:YAG, with a wavelength of around 2,100 nm).
How it works. The holmium is a pulsed laser, absorbed by the water in the tissue, with relatively shallow penetration and good coagulating ability. Applied to the enlarged turbinate, it reduces the tissue responsible for the swelling and, at the same time, coagulates the small vessels, which decreases bleeding during the procedure. Because it acts in a localized way, it seeks to preserve the lining mucosa and the nose’s humidifying function.
An interesting detail: since the holmium’s light is infrared and invisible, the device also projects a green aiming beam so the surgeon can see exactly where it will act. That is why, in surgical images, this laser appears green.
Advantages in this context. Two features stand out. The first is good hemostasis: by coagulating while it reduces the tissue, the procedure tends to involve little bleeding. The second is the durability of the results. In a long-term comparative study, subjective improvement in nasal breathing was reported by about 67.5% of patients treated with holmium and 74.4% of those treated with the diode laser, with objective improvement in airflow at both 6 months and 3 years. [1]
A striking point is that reducing the turbinate does not improve only the stuffy nose. By decreasing the volume of the mucosa that reacts to allergens and of the glands that produce secretion, the procedure tends to also reduce sneezing, runny nose, and itching, that is, the set of symptoms of allergic rhinitis flare-ups. A Japanese group followed patients for up to five years after laser turbinate surgery and observed sustained improvement in sneezing, runny nose, and obstruction, with a large proportion of them remaining off medication. [2] And a 2023 systematic review with meta-analysis, gathering 18 studies and more than 1,400 patients, confirmed that turbinate reduction significantly improves obstruction, runny nose, sneezing, and nasal itching, with the benefit maintained for more than a year. [3]
Despite this reduction of the turbinate and the improvement in obstruction and allergic symptoms, the allergy does not cease to exist. If the rhinitis is not controlled, the turbinate may swell again over time. For this reason, turbinoplasty is usually part of a plan, and long-term follow-up is important.
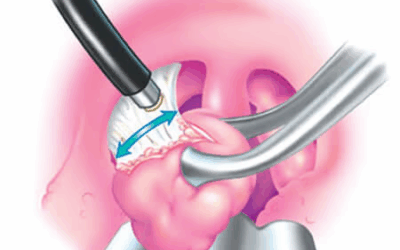
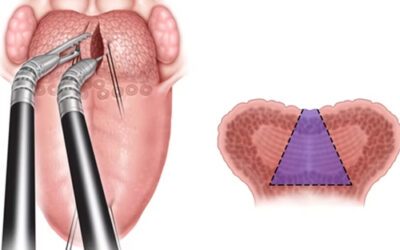
Blue laser (445 nm) in diseases of the larynx and vocal folds
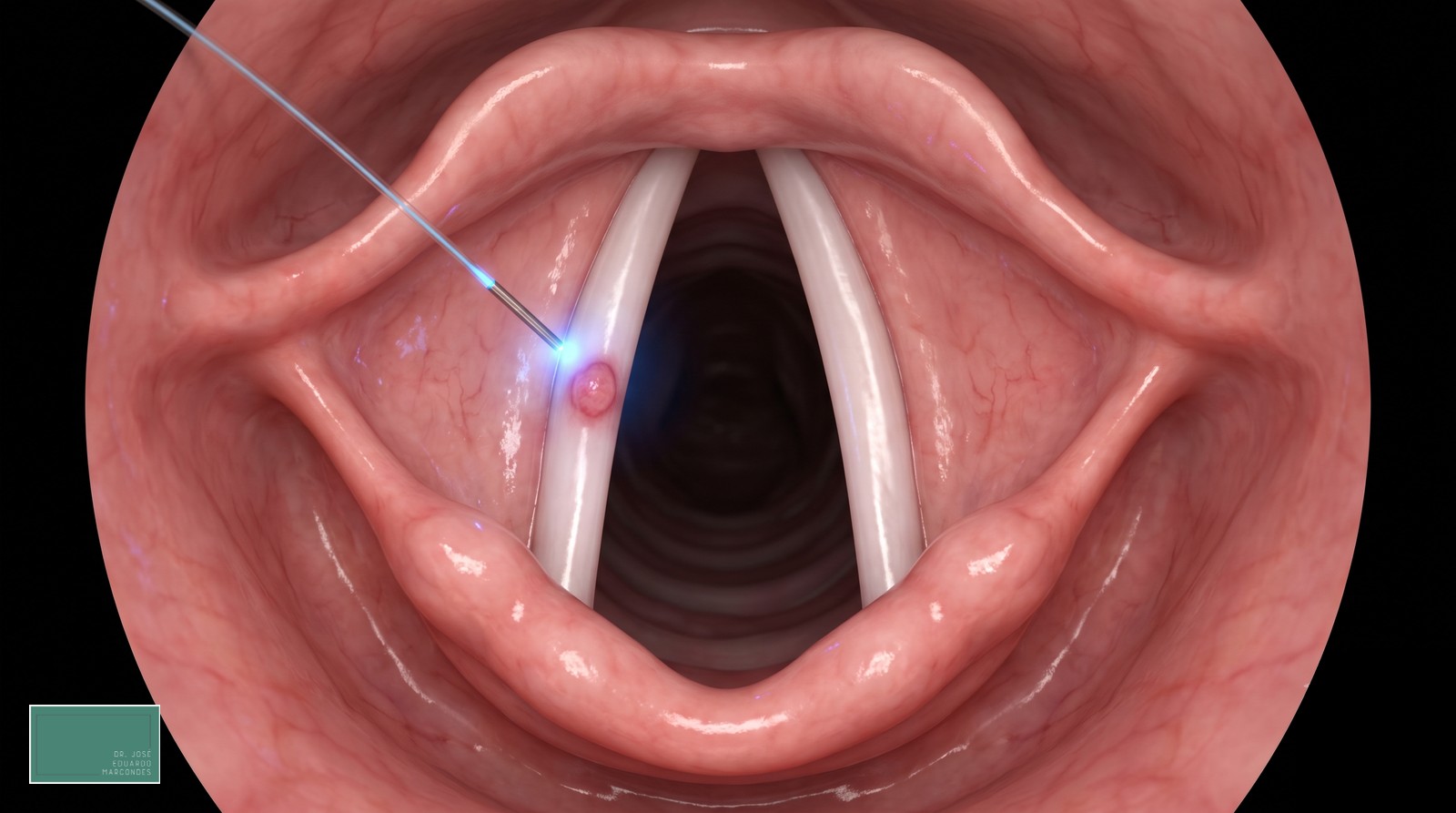
The larynx houses the vocal folds, delicate structures in constant motion that are responsible for producing the voice. Any lesion there, however small, can alter the voice and requires precise treatment, able to resolve the problem without harming the thin, layered tissue of the vocal fold. It is in this demanding setting that the blue laser (blue light, at 445 nm) has found a prominent role.
Why the target matters here. The blue laser’s main target is hemoglobin, so it acts preferentially on blood vessels. It happens that many vocal fold lesions are either vascular or fed by abnormal vessels. As it is absorbed by hemoglobin, the laser selectively coagulates these microvessels, treating the lesion with little bleeding and seeking to spare the vocal ligament and the deeper layers, which helps preserve the voice. This ability to act on vessels is what is called the photoangiolytic effect.
What can be treated. In the larynx, the blue laser has been used for a variety of lesions, among them [4][5]:
- vascular lesions of the vocal folds, such as varices, ectasias, and hemorrhagic polyps;
- Reinke’s edema;
- laryngeal papillomatosis (HPV-related lesions, which tend to recur);
- leukoplakia and early dysplastic lesions;
- granulomas.
Advantages in this context. Beyond coagulating, the blue laser also cuts, something the classic photoangiolytic lasers, such as the KTP, do not do. In laryngeal surgery, this combination has been described as bringing together, in a single device, the ability to cut and to treat the vessels. [4] Because it is delivered through a very thin fiber, it allows a precise and minimally invasive approach to vocal fold lesions, and the selective coagulation of the vessels improves visibility during the procedure. In practice, the blue laser has already been applied to different vocal lesions, such as polyps, Reinke’s edema, papilloma, and leukoplakia. [5] Because it is repeatable, it is also a useful option when the lesion tends to recur, as happens in papillomatosis.
The same caveat as in the other examples applies: the choice of laser and approach depends on the type of lesion, and the correct diagnosis always comes before the technology.
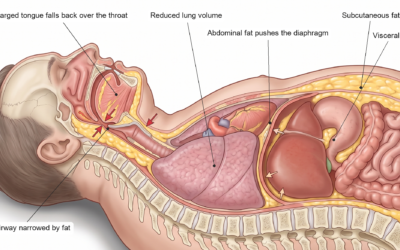
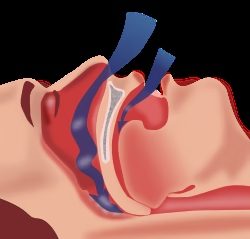
Fotona laser (Er:YAG) in snoring and sleep apnea

The third example again changes the objective. In the treatment of snoring and obstructive sleep apnea, the problem often lies in the laxity of the throat tissues, the soft palate, the uvula, and the walls of the pharynx, which vibrate (snoring) and, in some people, collapse and obstruct the airflow (apnea). The goal, in this case, is not to cut or remove tissue, but to tone it.
How it works. The Fotona laser, in the NightLase protocol, uses an erbium laser (Er:YAG, at 2,940 nm), in a mode called SMOOTH, with a non-ablative application. It heats the throat tissues in a controlled way, without cutting and without anesthesia. This heat causes the existing collagen fibers to contract and stimulates the production of new collagen over the following weeks. The tissue tends to become gradually firmer, with less tendency to vibrate and collapse during sleep.
Advantages and limits. It is an office-based procedure, painless, without cuts, and with no recovery time. A 2025 systematic review with meta-analysis concluded that the erbium laser is a safe and effective option in the short and medium term for selected patients with snoring or mild to moderate apnea, with benefits that usually last 1 to 2 years. [6] A randomized controlled trial, with a placebo group, also showed a significant reduction in snoring with the NightLase protocol, well tolerated. [7] A 4-year follow-up reinforced this profile over time. [8]
The Fotona laser works best in primary snoring and in mild to moderate apnea, and it does not replace CPAP in moderate to severe cases. The improvement, moreover, is usually clearer in the symptoms reported by the patient and normally requires booster sessions over time.
The three lasers side by side
The table below summarizes why each laser goes to a different task. Note that the logic is always the same: the wavelength defines the target, and the target defines the application.
| Laser | Wavelength | Main target | Predominant action | Highlighted application |
|---|---|---|---|---|
| Blue laser | 445 nm | hemoglobin and melanin | cuts and coagulates (photoangiolytic) | diseases of the larynx and vocal folds |
| Holmium (Ho:YAG) | 2,100 nm | water | coagulates and reduces volume | turbinoplasty (turbinate reduction) |
| Erbium (Er:YAG, Fotona) | 2,940 nm | water | heats without cutting (non-ablative) | snoring and apnea (palate and pharynx) |
Note that holmium and erbium have the same target (water) but produce quite different effects because of the wavelength, the pulse shape, and the mode of application. This shows that knowing the target is not enough: the “how” also counts.
Is the laser always the best option?
A laser is a tool, not a diagnosis. It can be a good choice in many situations, but the decision always depends on the cause of the problem. A few examples help to understand:
- If the nose is blocked because of a deviated septum, reducing only the turbinate with a laser may not solve it, because the main obstruction is in the bony and cartilaginous structure.
- If sleep apnea is severe, the treatment of choice remains CPAP or, in selected cases, surgery, not the laser.
- In several procedures, there are non-laser alternatives (such as radiofrequency and conventional surgical techniques), with good results.
For this reason, the right question is not “which is the best laser?” but “which is the best treatment for my case?” The answer comes from an evaluation that understands the origin of the symptom before choosing the technology.
Frequently asked questions
Is there a “best laser” for ENT?
No. Each laser has a target and a purpose. The one used to reduce turbinates is not the same as the one used to tone the throat for snoring, nor the most suitable for cutting soft tissue with bleeding control. The best laser is the one most appropriate to the objective of each case.
Does every laser treatment hurt or require anesthesia?
It depends on the procedure and the type of laser. The application of the Fotona laser for snoring, for example, is painless and does not require anesthesia, whereas procedures that reduce or remove tissue, such as turbinoplasty and laryngeal surgeries, require appropriate anesthesia, defined case by case at the evaluation.
Does the laser always cut or remove tissue?
No. Some lasers cut or reduce tissue (like the holmium and the blue laser), and others simply heat in a controlled way, without cutting (like the Fotona in non-ablative mode). They serve different purposes.
Does the laser used on the vocal fold harm the voice?
The goal is precisely the opposite: to treat the lesion while preserving as much of the healthy vocal fold tissue as possible. By acting selectively on the vessels, the blue laser seeks to spare the layers responsible for vibration and voice. Even so, every laryngeal procedure requires careful evaluation and technique, and voice recovery is monitored case by case.
Does the turbinate laser cure rhinitis?
No. Turbinoplasty reduces the obstruction caused by the enlarged turbinate, but the underlying rhinitis needs its own treatment. Without controlling the cause, the turbinate may swell again over time.
Does the Fotona laser replace CPAP?
Not always. In mild to moderate apnea, it can be an alternative or a complement. In moderate to severe apnea, CPAP or surgery remain the treatment of choice. The decision depends on the sleep study and on the individual evaluation.
Can anyone undergo a laser treatment?
The indication is always individual and defined after medical evaluation. There are situations that contraindicate each procedure, and the laser is not always the main path.
In summary
The laser is not a single technology, but a family of tools that differ by wavelength and by their target in the tissue. Holmium reduces turbinates with good hemostasis, the blue laser treats lesions of the larynx and vocal folds by coagulating the vessels while seeking to preserve the voice, and the Fotona laser tones the throat to help with snoring and mild to moderate apnea. Knowing these differences helps the patient understand the options, but the choice of the best approach always depends on the diagnosis.
If you have questions about nasal obstruction, snoring, sleep apnea, or about which treatment makes sense for your case, the path is an evaluation that identifies the cause before deciding on the technology.
Dr. José Eduardo Marcondes is a physician and otolaryngologist (ENT) (CRM SP 107711 | RQE 43840), working in nasal surgery and in the treatment of snoring and sleep apnea, seeing patients in Morumbi and Itaim (São Paulo) and in Alphaville (Barueri).
This content is informational and does not replace a medical consultation. References to studies are presented factually and do not constitute a promise of results.
References
Sroka R, Janda P, Killian T, Vaz F, Betz CS, Leunig A. Comparison of long term results after Ho:YAG and diode laser treatment of hyperplastic inferior nasal turbinates. Lasers in Surgery and Medicine. 2007;39(4):324-331. doi:10.1002/lsm.20479.
Takeno S, Nakashimo Y, Ishino T, Miyahara N, Goh K, Noda N, Hirakawa K. Long-Term Results after Carbon Dioxide Laser Surgery of the Inferior Turbinate for Perennial Allergic Rhinitis. Nihon Bika Gakkai Kaishi (Japanese Journal of Rhinology). 2011;50(1):7-12. doi:10.7248/jjrhi.50.7.
Park SC, Kim DH, Jun YJ, Kim SW, Yang HJ, Yang SI, Kim HJ, Kim DK. Long-term Outcomes of Turbinate Surgery in Patients With Allergic Rhinitis: A Systematic Review and Meta-analysis. JAMA Otolaryngology-Head and Neck Surgery. 2023;149(1):15-23. doi:10.1001/jamaoto.2022.3567.
Hess MM, Fleischer S, Ernstberger M. New 445 nm blue laser for laryngeal surgery combines photoangiolytic and cutting properties. European Archives of Oto-Rhino-Laryngology. 2018;275(6):1557-1567. doi:10.1007/s00405-018-4974-8.
Hamdan AL, Ghanem A. Un-sedated Office-Based Application of Blue Laser in Vocal Fold Lesions. Journal of Voice. 2023;37(5):785-789. doi:10.1016/j.jvoice.2021.03.031.
Dembicka-Maczka D, et al. Effectiveness of the Er:YAG Laser in Snoring Treatment Based on Systematic Review and Meta-Analysis Results. Journal of Clinical Medicine. 2025;14(12):4371. doi:10.3390/jcm14124371.
Picavet VA, et al. Treatment of snoring using a non-invasive Er:YAG laser with SMOOTH mode (NightLase): a randomized controlled trial. European Archives of Oto-Rhino-Laryngology. 2022;280(1):307-312. doi:10.1007/s00405-022-07539-9.
Frelich H, et al. Erbium:Yttrium Aluminum Garnet (Er:YAG) Laser: A Minimally Invasive Treatment Method in Selected Patients with Impaired Breathing During Sleep. Photobiomodulation, Photomedicine, and Laser Surgery. 2023;41(8):415-421. doi:10.1089/photob.2022.0144.
Read also:
About the author
Dr. José Eduardo Marcondes
Otolaryngologist (ENT) · CRM-SP 107.711 · RQE 43.840
Trained and completed his residency at Escola Paulista de Medicina (UNIFESP), with more than two decades of experience. A pioneer in the use of robotic surgery (TORS) for sleep apnea. Member of the clinical staff at Hospital Albert Einstein, Vila Nova Star and São Luiz. Member of ABORL-CCF.
Learn about his full career → · Schedule an appointment on WhatsApp