Sleep apnea and excess weight often go hand in hand, and this is no coincidence. The two conditions feed each other: extra weight favors apnea, and apnea, in turn, makes losing weight harder. It is a true vicious cycle, and understanding it helps explain why treating only one side often fails to solve the problem.
In this article on sleep apnea and obesity, the goal is educational: to show how obesity worsens apnea, how apnea worsens obesity, and why breaking this cycle requires looking at both problems at the same time. At the end, we discuss the available treatments and why the so-called weight-loss injections (GLP-1 medications) have become an important tool against both diseases.
What obstructive sleep apnea is
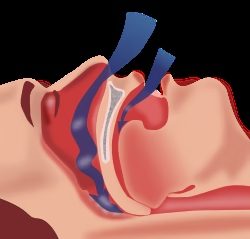
During sleep, the muscles of the throat relax. In people with a narrower airway or more lax tissues, this relaxation can temporarily close off the passage of air, interrupting breathing for a few seconds, several times a night. Each pause prompts the brain to react with a micro-arousal in order to resume breathing. Sleep becomes fragmented, the body does not truly rest, and blood oxygen levels swing throughout the night.
This is obstructive sleep apnea. Among the factors that favor its onset, excess weight is one of the most important, and also one of the most reversible.
Focus 1: how obesity worsens apnea
Excess weight works against nighttime breathing through several pathways at once.
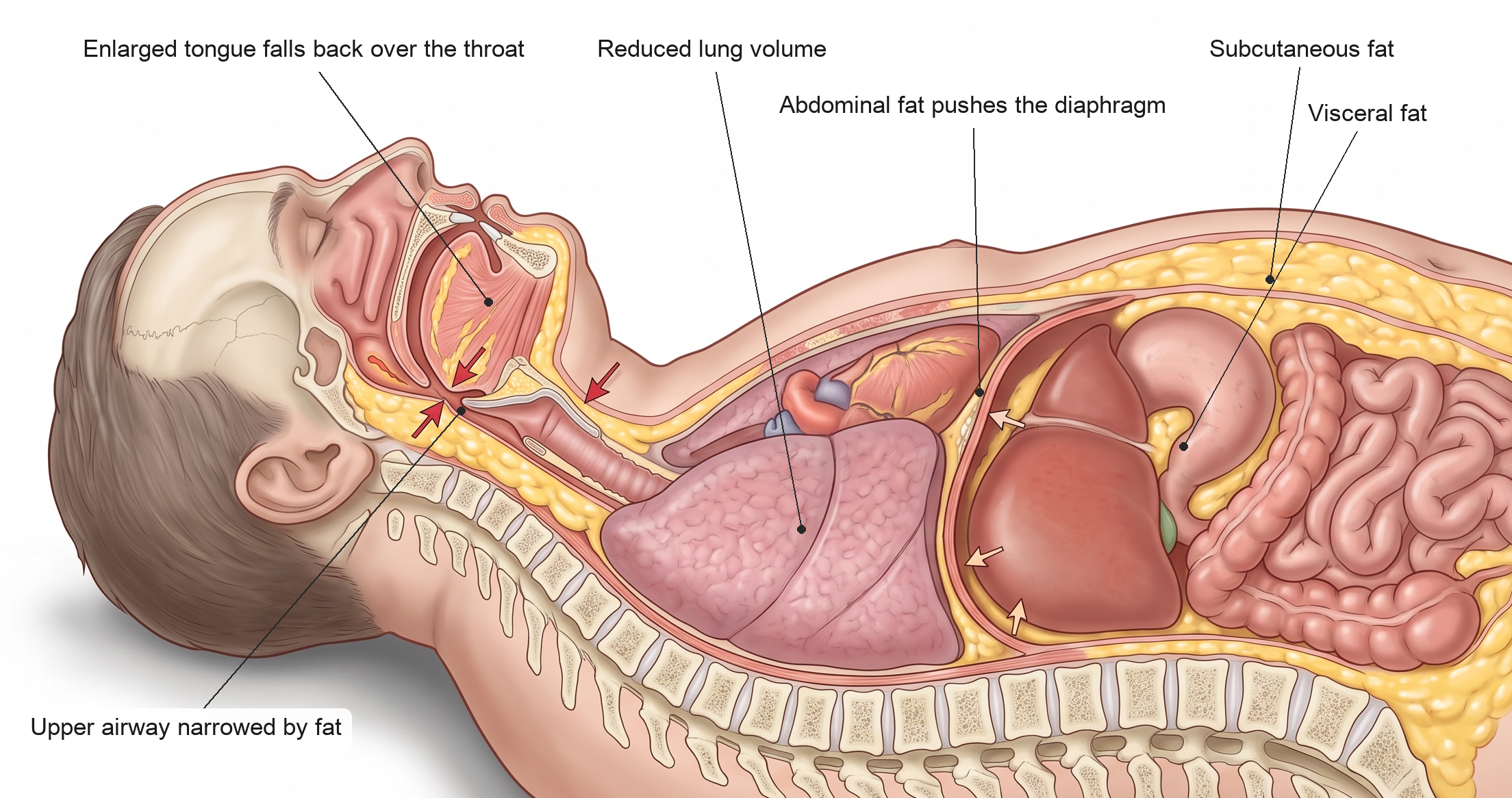
- Fat around the throat. Fat that builds up in the neck and along the walls of the pharynx narrows the space through which air passes. A tighter airway collapses more easily when the muscles relax during sleep.
- Fat at the base of the tongue. MRI studies show that people with obesity tend to accumulate fat in the tongue itself, which becomes larger and heavier and falls back over the throat when lying down.
- Abdominal fat. Belly fat pushes the diaphragm upward and reduces the volume of air the lungs can hold, especially when lying down. Less inflated lungs “pull” less on the airway from within, leaving it more prone to closing.
- Inflammation and fluid retention. Excess fat tissue keeps the body in a state of low-grade inflammation and promotes fluid buildup, which at night can shift to the neck and worsen the obstruction.
It is no coincidence that the relationship between weight and apnea is well documented. A landmark population study showed that a change of about 10% in body weight is associated with substantial changes in the severity of apnea: gaining weight worsens it, and losing weight improves the number of breathing pauses per hour of sleep.
Focus 2: how apnea worsens obesity
What many people do not realize is that this is a two-way street. Untreated apnea also pushes the body toward weight gain and makes losing weight harder.
- Fragmented sleep disrupts hunger. Sleep deprivation and fragmentation alter two hormones that control appetite: they raise ghrelin (which drives hunger) and lower leptin (which signals fullness). The result is more hunger, more craving for calorie-dense foods, and more difficulty stopping eating.
- Insulin resistance. Poor nights of sleep and repeated drops in oxygen worsen the way the body handles sugar, promoting insulin resistance, fat accumulation, and the risk of type 2 diabetes.
- Fatigue that reduces energy expenditure. People who sleep poorly wake up exhausted, with less drive to exercise and move throughout the day. Less activity means fewer calories burned.
- Hormonal stress. Poor sleep and oxygen swings activate the stress system and raise cortisol, a hormone that also promotes fat accumulation, mainly in the abdominal area.
In other words, apnea creates exactly the hormonal and behavioral environment that makes gaining weight easier.
The vicious cycle
Put the two sides together and the problem becomes clear. Excess weight narrows and overloads the airway, which causes or worsens apnea. Apnea fragments sleep, disrupts hunger hormones, increases insulin resistance, and drains the energy needed to exercise, which further promotes weight gain. More weight, more apnea. More apnea, more weight.
This is why many people feel “stuck”: they diet, but poor sleep sabotages the effort; or they treat only the sleep, but their weight keeps the airway compromised. Breaking this cycle usually requires acting on both fronts at once, and this is where modern treatment has made considerable progress.
How apnea is treated today
There is no single treatment that works for everyone. The approach depends on the severity of the apnea, the anatomy of the airway, and each person’s associated factors. The main options are:
- CPAP. The device that keeps the airway open with a flow of air throughout the night. It remains the treatment of choice for severe apnea.
- Treating the nose. Correcting obstructions such as a deviated nasal septum, enlarged turbinates, or rhinitis improves breathing and adaptation to other treatments.
- Oral appliance. A device that slightly advances the lower jaw and widens the space in the throat, useful in mild to moderate cases.
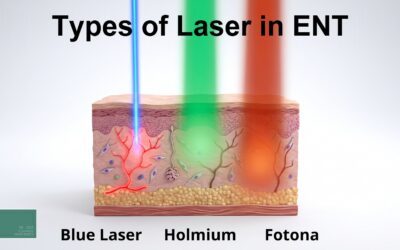
- Fotona laser. The NightLase protocol, a laser treatment with no cutting, can tone the tissues of the throat in selected cases of snoring and mild to moderate apnea.
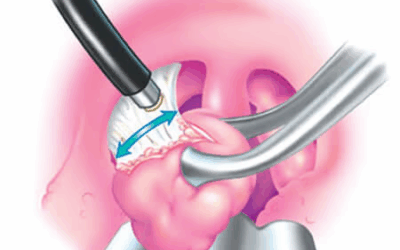
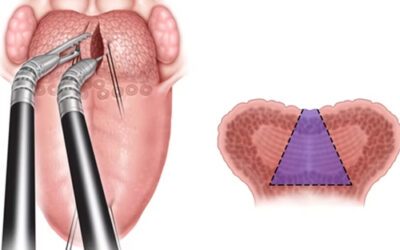
- Surgery. Indicated in specific situations, according to the point of obstruction identified during the evaluation.
- Weight management. As we have seen, it is a central piece. Losing weight reduces the severity of apnea and, in some cases, can even resolve mild forms.
Weight, in fact, has always been on this list, but for a long time it was also the hardest part to treat. It was precisely here that an important development emerged.
Weight-loss injections: one weapon against both conditions
These weight-loss injections are medications from the class of GLP-1 receptor agonists (such as semaglutide) and, more recently, dual GLP-1/GIP receptor agonists (such as tirzepatide). They act on the brain and the digestive system by increasing satiety and reducing hunger, which leads to significant and sustained weight loss.
The interesting point for people with apnea is that these medications target the very root of the vicious cycle: excess weight. And there is direct evidence of this. In 2024, a large clinical trial called SURMOUNT-OSA, published in the New England Journal of Medicine, evaluated tirzepatide in adults with obesity and moderate-to-severe obstructive sleep apnea. The result was a significant reduction in the number of breathing pauses per hour of sleep (the apnea-hypopnea index, or AHI, which measures the severity of apnea), along with weight loss, both in those using CPAP and in those who were not.
In practice, this means that treating weight with these medications may improve the apnea itself, while also reducing risks linked to obesity, such as diabetes and cardiovascular disease. A single line of treatment acting on both conditions at once.
Two important caveats, however. First, these injections are not a miracle and do not, on their own, replace the other treatments: in many cases they are added to CPAP and the other measures rather than eliminating them. Second, they are medications with their own indications, contraindications, and side effects, whose prescription and follow-up are the responsibility of the physician in charge of weight treatment, usually the endocrinologist or an obesity medicine physician.
The best path is team-based care. The otolaryngologist (ENT) evaluates and treats the airway and the apnea; the obesity specialist manages weight loss, with or without medication; and the two work together to break the vicious cycle. Each piece in its place, with a shared goal: to give the patient real sleep and more balanced health.
Frequently asked questions
Does losing weight cure sleep apnea?
It depends on the case. Weight loss reduces the severity of apnea in almost everyone and, in mild cases linked to excess weight, it may even resolve it. In moderate-to-severe apnea, it usually helps considerably, but often needs to be combined with other treatments, such as CPAP.
Do only people with obesity have apnea?
No. Excess weight is one of the main risk factors, but lean people can also have apnea, due to features of the anatomy of the face and throat, nasal obstruction, or hormonal factors. That is why diagnosis depends on assessment, and not on weight alone.
Does sleep apnea cause weight gain?
It can contribute, yes. By fragmenting sleep, apnea disrupts appetite hormones (increasing hunger and reducing satiety), worsens insulin resistance, and causes fatigue that lowers the drive to exercise. Together, these factors promote weight gain and help explain why treating apnea often makes weight management easier.
Why do I sleep poorly and still gain weight?
The fragmented sleep of apnea disrupts appetite hormones: it increases hunger, reduces satiety, and worsens how the body handles sugar. Combined with the fatigue that lowers the drive to exercise, this promotes weight gain even when you are making an effort to lose weight.
Do weight-loss injections treat apnea?
Indirectly, yes. By promoting weight loss, medications such as tirzepatide reduced the severity of apnea in recent studies. They act on the cause (excess weight), but they do not replace assessment of the airway nor, in many cases, CPAP. The indication is always individual and made by a physician.
Who prescribes weight-loss injections?
Prescription and follow-up are the responsibility of the physician in charge of weight treatment, usually the endocrinologist or an obesity medicine physician. The otolaryngologist (ENT) takes care of the airway and the apnea. The ideal is teamwork, with the specialists complementing one another.
How do I know if I have apnea?
Warning signs include loud snoring, breathing pauses noticed by a bed partner, unrefreshing sleep, fatigue, and daytime sleepiness. Diagnosis begins with a clinical and airway assessment and is usually confirmed by polysomnography, the sleep study.
It’s worth talking about your case
If you live with snoring, unrefreshing sleep, daytime fatigue, or difficulty losing weight, there may be sleep apnea behind it, feeding this cycle. The good news is that the cycle can be broken, and the sooner the origin of the problem is understood, the better the results.
Dr. José Eduardo Marcondes is a physician and otolaryngologist (ENT) (CRM SP 107711 | RQE 43840), focusing on nasal surgery and the treatment of snoring and sleep apnea, seeing patients in Morumbi and Itaim (São Paulo) and in Alphaville (Barueri). If it makes sense for you, book a consultation so we can talk about your case, ideally as part of integrated care alongside weight management.
References
- Peppard PE, Young T, Palta M, Dempsey J, Skatrud J. Longitudinal study of moderate weight change and sleep-disordered breathing. JAMA. 2000;284(23):3015-3021. doi:10.1001/jama.284.23.3015.
- Malhotra A, Grunstein RR, Fietze I, et al. Tirzepatide for the treatment of obstructive sleep apnea and obesity (SURMOUNT-OSA). New England Journal of Medicine. 2024;391(13):1193-1205. doi:10.1056/NEJMoa2404881.
- Spiegel K, Tasali E, Penev P, Van Cauter E. Sleep curtailment in healthy young men is associated with decreased leptin levels, elevated ghrelin levels, and increased hunger and appetite. Annals of Internal Medicine. 2004;141(11):846-850. doi:10.7326/0003-4819-141-11-200412070-00008.
- Schwartz AR, Patil SP, Laffan AM, Polotsky V, Schneider H, Smith PL. Obesity and obstructive sleep apnea: pathogenic mechanisms and therapeutic approaches. Proceedings of the American Thoracic Society. 2008;5(2):185-192. doi:10.1513/pats.200708-137MG.
This content is informational and does not replace a medical consultation.
Read also:
About the author
Dr. José Eduardo Marcondes
Otolaryngologist (ENT) · CRM-SP 107.711 · RQE 43.840
Trained and completed his residency at Escola Paulista de Medicina (UNIFESP), with more than two decades of experience. A pioneer in the use of robotic surgery (TORS) for sleep apnea. Member of the clinical staff at Hospital Albert Einstein, Vila Nova Star and São Luiz. Member of ABORL-CCF.
Learn about his full career → · Schedule an appointment on WhatsApp