Few decisions leave parents as uncertain as the prospect of their child undergoing surgery. If you have reached this page after nights spent listening to your child snore, watching them sleep with an open mouth, or after yet another bout of sore throat, it is only natural to feel that mix of worry and doubt: “does my child really need an operation?”
The good news is that this decision does not have to be made in the dark. There are well-established criteria, based on medical guidelines, that help separate the cases worth watching and waiting from those in which surgery tends to bring a real benefit. This article explains, in plain language, what the adenoid and tonsils are, why they enlarge, which signs deserve attention, and how the otolaryngologist (ENT) reaches a conclusion about whether or not to operate.
The aim here is to give you quality information so you can have a calmer conversation during the appointment and better understand what is happening with your child.

What are the adenoid and the tonsils?
The adenoid and tonsils are defense tissues made up of immune system cells. They act as a kind of “watch post” at the entrance to the airway, helping the body recognize viruses and bacteria, especially in the first years of life.
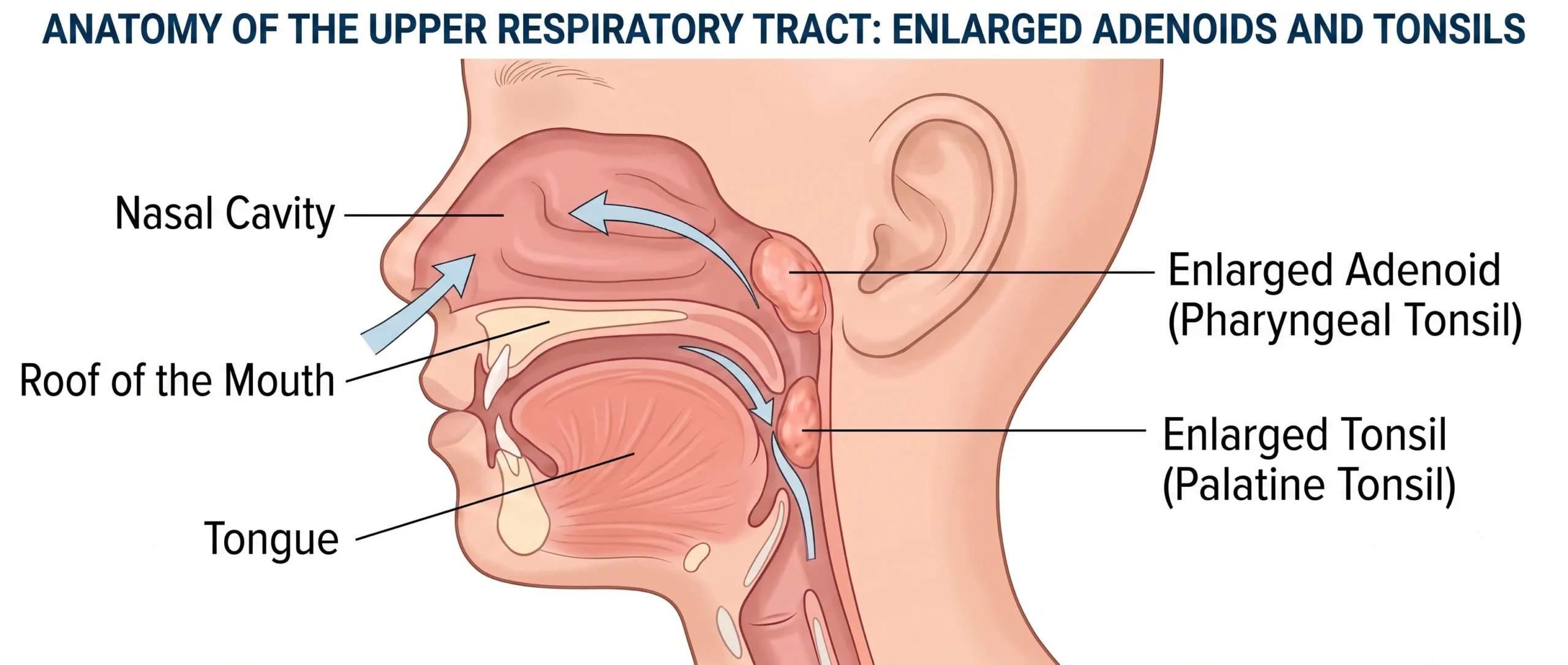
- Tonsils (or palatine tonsils): located on the sides of the throat. They are those two little “balls” you can see when the child opens their mouth wide.
- Adenoid (or pharyngeal tonsil): more hidden, at the back of the nose, behind the roof of the mouth. It cannot be seen with the naked eye in an ordinary appointment, which is why many parents have never seen it. It is like a third tonsil at the back of the nose.
Although they are part of the defense system, the body has many other immune mechanisms. For this reason, when surgery is needed, removing these tissues does not leave the child “defenseless,” as is often feared.
Why do the adenoid and tonsils enlarge?
It is common for these tissues to grow naturally in the first years of life, precisely during the stage when the child has the most contact with viruses and bacteria (daycare, school, older siblings). This enlargement is often temporary and tends to recede as the child grows.
The problem appears when the enlargement is great enough to interfere with breathing and sleep, or when the tonsils become infected repeatedly. Some children have an individual tendency toward larger tissues; respiratory allergies and recurrent infections can also contribute.
It is worth separating two scenarios that parents often blur together:
- Enlarged size that obstructs (large adenoid and/or tonsils that make breathing and sleeping difficult).
- Recurrent infections (frequent tonsillitis), which is a different problem, even though it sometimes occurs in the same child.
The criteria for considering surgery differ in each of these scenarios, as you will see below.
Which signs in children deserve parents’ attention?
The signs vary according to what is enlarged and by how much. We have gathered the most common ones below. Seeing one or another isolated item does not mean surgery is indicated, but the presence of several signs, in a persistent way, is a good reason to seek an evaluation.
Signs linked to obstruction and sleep (large adenoid and tonsils)
- Frequent snoring, several nights a week.
- Mouth breathing, while asleep and sometimes awake; a child who sleeps with an open mouth or keeps the mouth open during the day.
- Restless sleep, with frequent position changes, awakenings, and the feeling that the child “doesn’t rest.”
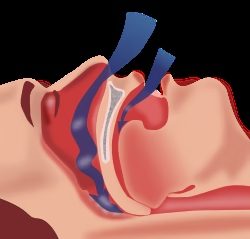
- Pauses in breathing during sleep, sometimes followed by a gasp or choking sound (the sign that worries parents most, and rightly so).
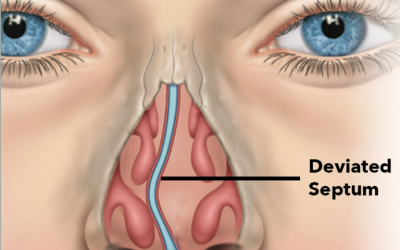
- A nasal-sounding voice (as if always “stuffed up”) and difficulty breathing through the nose.
- Daytime sleepiness or irritability, difficulty concentrating, and an impact on school performance.
- Bedwetting that persists or returns, which in some children is related to the sleep disorder.
- In more prolonged cases, changes in growth or in the shape of the face and dental arch, linked to continuous mouth breathing, along with dental or bite changes.
Together, these signs may point to what we call sleep-disordered breathing, which ranges from simple snoring to obstructive sleep apnea (OSA) in children, when there are pauses and a drop in sleep quality and oxygenation. This is a topic that deserves attention because sleep is essential to a child’s development. (You can read more about this in our article on sleep apnea in children.)

Signs linked to recurrent infections (tonsils)
- Recurrent tonsillitis: frequent episodes of sore throat with fever, exudate (white spots) on the tonsils, and swollen glands in the neck.
- Recurrent school absences and repeated use of antibiotics over the course of the year.
If the main complaint is repeated sore throats, it is worth understanding the situation better on our page about tonsillitis and sore throat.
Signs linked to the ear
- Recurrent ear infections (otitis media) or fluid behind the eardrum, which may be related to an enlarged adenoid.
- A sense of muffled hearing or asking to turn up the TV volume, which, in children, sometimes goes unnoticed.
When is it a matter of simply monitoring, and when is investigation needed?
Not every instance of snoring, and not every large tonsil, means surgery. In many cases, the most sensible approach is to monitor, because these tissues may recede as the child grows.
In general, it usually makes sense to observe and reassess when:
- snoring is occasional, linked to colds or allergy flare-ups, and improves outside those periods;
- there are no pauses in breathing or signs of poor-quality sleep;
- throat infections are infrequent;
- the child grows, sleeps, and functions well day to day.
On the other hand, it is usually worth investigating with an otolaryngologist when there is:
- frequent snoring accompanied by mouth breathing and restless sleep;
- reports of pauses in breathing during sleep;
- an impact on behavior, attention, or school performance;
- repeated throat infections over the course of the year;
- recurrent ear infections or suspected hearing loss.
The decision between monitoring and operating is individual and takes into account the intensity of the symptoms, the child’s age, the impact on their life, and the physical examination, not just the size of the tissues in isolation.
How does the otolaryngologist evaluate the child?
The evaluation begins with a detailed conversation (clinical history) and the physical examination. Often, this combination already guides the approach well. Depending on the case, the physician may turn to:
- Examination of the throat and nose, to estimate the size of the tonsils and assess breathing.
- Flexible nasolaryngoscopy (an examination with a thin, flexible camera) or, in some cases, a lateral neck radiograph, to assess the adenoid, which is normally not visible to the naked eye. The choice of examination depends on the child’s age and cooperation.
- Polysomnography (sleep study): this is the reference test to confirm and measure the severity of obstructive sleep apnea. According to the guidelines, it is usually indicated when there is doubt about the real need to operate, or in children with conditions that increase risk (for example, very young age, obesity, Down syndrome, or craniofacial or neuromuscular abnormalities). Not every child needs this test before surgery.
- Hearing assessment, when ear infections or hearing loss are suspected.
The goal of this stage is to understand the overall picture, not just “how big it is”, so that the indication, if any, is genuinely well-founded.
When is surgery usually indicated in children?
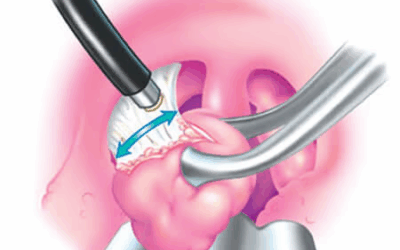
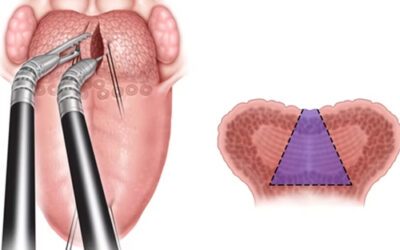
The most common surgery in this context is adenotonsillectomy (removal of the adenoid and tonsils). In some cases, only the adenoid is removed (adenoidectomy) or only the tonsils (tonsillectomy), depending on the evaluation.
Recognized medical guidelines (such as those of the American Academy of Otolaryngology – AAO-HNS) organize the indications around two main reasons. It is worth stressing that these criteria guide the consultation, but the surgical indication is always an individual decision, made case by case between the family and the physician, not an automatic recommendation for every child with enlarged adenoids or tonsils.

1. Airway obstruction and sleep apnea
When enlargement of the adenoid and/or tonsils causes obstructive sleep apnea or sleep-disordered breathing with an impact on the child, surgery is considered the first-line treatment, according to the leading guidelines. In these cases, improving sleep and breathing is usually the main goal.
2. Recurrent throat infections
For recurrent tonsillitis, the guidelines adopt quite objective criteria (known as the Paradise criteria) to help with the decision. In general, surgery tends to be considered when the number of well-documented sore-throat episodes is:
- 7 or more episodes in 1 year; or
- 5 or more episodes per year over the last 2 years; or
- 3 or more episodes per year over the last 3 years.
For this purpose, each episode must have been a sore-throat episode accompanied by at least one of the following findings: fever above 38.3 °C, swollen glands in the neck (tender lymph nodes), exudate on the tonsils, or a positive test for streptococcus bacteria (group A Streptococcus).
Below these numbers, the guidelines recommend watching and waiting rather than operating, since in these cases surgery may not bring as much benefit. This is not a rigid, automatic rule: particular situations (such as severe tonsillitis, recurrent abscesses, or other factors) can change the assessment, always on an individual basis.
In short: the number of episodes is not everything, but it is an important starting point. That is why it is worth noting down the dates and symptoms of your child’s tonsillitis over time, this history is a great help to the physician in deciding.
What is recovery from surgery usually like?
Adenotonsillectomy is usually a short procedure, generally with discharge on the same day or after a night of observation, depending on the child’s age, the case, and the team’s assessment.
General points that are usually part of the postoperative period (always according to the physician’s individual guidance):
- Sore throat in the first few days, which is expected and managed with medication.
- A preferably cold, soft, and light diet at first, gradually returning to normal.
- Relative rest and a temporary break from school and more intense physical activities for a few days.
- Attention to warning signs indicated by the team, such as bleeding, a situation in which medical care should be sought.
Today there is the option of using certain technologies that improve the quality and safety of the postoperative period, such as radiofrequency. To learn more about this advance in surgery, visit my page on tonsillectomy with coblation.
Like any surgery, adenotonsillectomy has benefits and also risks, which must be explained and weighed case by case. There is no procedure without risks, and the decision must always weigh what is gained against what is avoided. Follow-up after surgery is an important part of the process.
Parents’ frequently asked questions (FAQ)
Is it normal for a child to snore?
Snoring now and then, during a cold, can happen. What deserves attention is frequent snoring, especially when accompanied by mouth breathing, restless sleep, or pauses in breathing. In these cases, it is worth seeking an evaluation.
Do enlarged adenoids and tonsils always need surgery?
No. Many cases are monitored over time, because these tissues may recede as the child grows. Surgery is considered when there is significant obstruction of sleep/breathing or recurrent infections within certain criteria.
Does removing the adenoid and tonsils weaken a child’s immunity?
The body’s defense system is broad and relies on several other organs and mechanisms. When surgery is well indicated, removing these tissues does not usually compromise a child’s immunity in any meaningful way.
What is the difference between adenoidectomy, tonsillectomy, and adenotonsillectomy?
Adenoidectomy is the removal of the adenoid only; tonsillectomy, of the tonsils only; and adenotonsillectomy, of both. What is removed depends on the evaluation of each child.
Do snoring and mouth breathing improve after surgery?
When the problem is caused mainly by the enlargement of these tissues, the tendency is for significant improvement in breathing and sleep. In some children, especially when there are other factors (such as obesity), follow-up and additional measures may be needed. The individual evaluation is what defines a realistic expectation.
Is there a right age to operate?
There is no single age. The decision considers the symptoms, the impact on the child, and the otolaryngologist’s evaluation. In very young children, additional care is usually taken during the investigation.
Can it be treated without surgery?
In some cases, especially milder ones or those linked to allergy, monitoring and medical treatment of the associated causes (such as rhinitis) may be enough. The approach depends on the case.
When to seek an evaluation?
If your child snores frequently, sleeps with an open mouth, has restless sleep, shows pauses in breathing, or has recurrent tonsillitis, it is worth talking to an otolaryngologist. A careful evaluation helps to determine, with sound judgment, whether the best path is to monitor or to operate, and to lift from parents the burden of deciding on their own.
To better understand enlarged adenoids in childhood, you can also read our page on adenoid hypertrophy in children and, if surgery is under discussion, the page on adenotonsillectomy. There is also content dedicated to adenoid and tonsil surgery in children.
Dr. José Eduardo Merighe Marcondes — PHYSICIAN (CRM SP 107711, RQE 43840), otolaryngologist, treats children and adults in Morumbi and Itaim (São Paulo-SP) and in Alphaville (Barueri-SP), with a focus on snoring and sleep apnea, including in childhood. Book a Consultation.
This content is informational and does not replace a medical consultation.
Read also:
About the author
Dr. José Eduardo Marcondes
Otolaryngologist (Physician) · CRM-SP 107.711 · RQE 43.840
Trained and resident at Escola Paulista de Medicina (UNIFESP), with more than two decades of experience. A pioneer in the use of robotic surgery (TORS) for sleep apnea. Member of the clinical staff at Hospital Albert Einstein, Vila Nova Star, and São Luiz. Member of ABORL-CCF.