“Doctor, can sleep apnea be cured?” This is one of the most frequent questions in the office, and the answer is: it depends on the cause and the severity. Sleep apnea always has effective treatment and, in specific situations, a real cure. In other cases, the goal is full control of the problem, which already transforms sleep, energy, and the health of those who live with it.
In this article, we explain the types of apnea, what leads a person to develop the problem, how to know whether you have it, when the condition is considered severe, and, above all, in which situations we can speak of a cure and in which the path is control.

What sleep apnea is
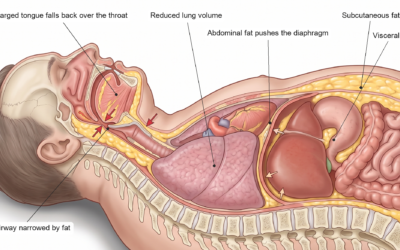
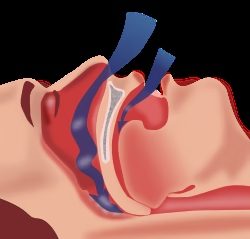
During sleep, the muscles of the throat relax. In people with a narrower airway or more lax tissues, this relaxation can close off the passage of air for a few seconds, several times a night. Each pause forces the brain into a micro-arousal to resume breathing. The result is fragmented sleep, blood oxygen swinging up and down, and a body that never truly rests.
This is obstructive sleep apnea, the most common form of the disease. It is far more frequent than people think: in the EPISONO study, carried out in the city of São Paulo, about one third of adults (32.8%) had sleep apnea to some degree. If you want to understand in detail what the pauses do to the body, it is worth reading the article on the physiology of sleep apnea.
What are the three types of apnea?
There are three types of sleep apnea, distinguished by the mechanism that interrupts breathing during the night:
| Type | What happens | How common |
|---|---|---|
| Obstructive apnea | The airway closes in the throat, but the body keeps trying to breathe. It is the focus of this article. | By far the most common type. |
| Central apnea | The brain briefly stops sending the command to breathe; the throat is not the problem. It tends to be associated with heart and neurological conditions. | Rarer. |
| Mixed apnea | It combines both mechanisms in the same event: it starts as central and ends as obstructive. | Less frequent. |
Telling the types apart matters because the treatment changes. Polysomnography, the sleep study, is what makes that distinction.
What leads a person to have sleep apnea?
In obstructive apnea, the problem comes from a simple equation: a narrow airway plus tissues that relax too much during sleep. Several factors feed into that equation:
- Excess weight. It is the most important risk factor and one of the most reversible. Fat in the neck, tongue, and abdomen narrows and overloads the airway. We explain this mechanism in detail in the article on sleep apnea and obesity.
- Anatomy of the face and throat. A receding chin, large tonsils, a bulky tongue, and a low palate reduce the space through which air passes. That is why lean people can also have apnea.
- Nasal obstruction. A deviated septum, enlarged turbinates, and rhinitis make breathing through the nose harder and push the person toward mouth breathing, which destabilizes the airway during sleep.
- Age and sex. Apnea becomes more common with age, as muscle tone is naturally lost. Men are more affected, but the difference narrows after menopause, as we show in the article on sleep apnea in men and women.
- Alcohol, smoking, and sedatives. They relax the throat muscles further or inflame the airway.
- Hormonal factors. Hypothyroidism and other hormonal changes can also contribute.
What makes apnea worse?
Even in people already diagnosed, some habits worsen the breathing pauses: gaining weight, drinking alcohol at night, smoking, taking sleeping pills on your own, sleeping on your back, and leaving the nose obstructed without treatment. The good news is that all these points can be worked on, and each of them improves the outcome of any treatment.
How do I know if I have sleep apnea?
The most common signs appear at two moments. At night: loud, frequent snoring, breathing pauses noticed by a bed partner, choking or a smothering sensation, restless sleep, and repeated trips to the bathroom. During the day: waking up tired even after hours in bed, morning headache, sleepiness, irritability, and a decline in memory and concentration.
When these signs are present, the way forward is an evaluation with an otolaryngologist (ENT), who examines the nose and throat (usually with flexible nasolaryngoscopy) to identify where the obstruction lies. The diagnosis is confirmed by polysomnography, the sleep study, which can be done in a lab or, in selected cases, at home.

When is apnea severe?
Severity is measured by the AHI, the apnea-hypopnea index, which counts the breathing pauses per hour of sleep: up to 5 is considered normal, 5 to 15 is mild apnea, 15 to 30 is moderate, and above 30 is severe.
The number, however, is not everything. The drop in oxygen during events, the degree of daytime sleepiness, the person’s occupation (think of someone who drives or operates machinery), and the presence of conditions such as high blood pressure, diabetes, and arrhythmias also weigh on how and how urgently to treat.
So, can sleep apnea be cured?
Now for the full answer. Sleep apnea can be cured in specific situations, when there is a well-defined cause that can be corrected:
- In children, the most common cause is enlargement of the tonsils and adenoid, and surgery resolves the large majority of cases.
- In adults with mild apnea linked to excess weight, consistent weight loss can normalize the sleep study.
- In selected cases, snoring and apnea surgery corrects the points of airway obstruction (nose, palate, pharyngeal walls, and base of tongue) and can bring the AHI down to normal levels. The result depends greatly on patient selection and the site of obstruction, which is why a detailed evaluation matters so much.
In most moderate and severe cases, the term we use is not cure, but control. CPAP, for example, eliminates the breathing pauses while it is in use, with an excellent effect on symptoms and quality of life. It is similar to what happens with high blood pressure: treatment does not make the predisposition disappear, but it restores health and keeps complications away. And control done well, in practice, means sleeping and living like someone who does not have the disease.
Be wary of any promise of a guaranteed cure for apnea. Serious medicine works with individual assessment, and the right treatment for one person may be wrong for another.
What are the treatments for sleep apnea?
The plan is always individual and, often, combines more than one front:
- CPAP. A device that keeps the airway open with air pressure. It is the treatment of choice for severe apnea and very effective when well tolerated.
- Oral appliance. It slightly advances the lower jaw and widens the space in the throat. Useful in mild to moderate cases and for those who do not adapt to CPAP.
- Treating the nose. Correcting a deviated septum, enlarged turbinates, and rhinitis improves breathing, snoring, and adaptation to CPAP.
- Speech therapy (myofunctional therapy). Exercises that strengthen the muscles of the tongue, palate, and pharynx.
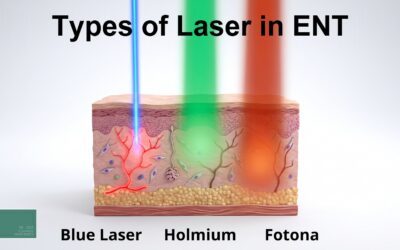
- Fotona laser. The NightLase protocol, a laser treatment with no cutting, tones the tissues of the throat in selected cases of snoring and mild to moderate apnea.
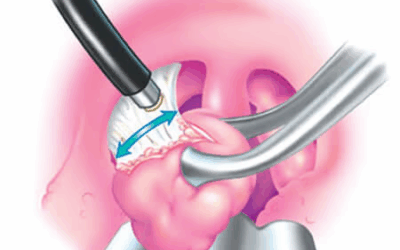
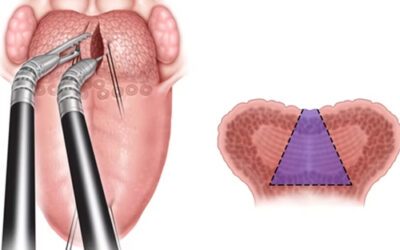
- Surgery. From nasal procedures to pharyngoplasty and robotic base-of-tongue surgery (TORS), indicated according to the point of obstruction identified during the evaluation.
- Weight management. A central piece in people with excess weight, with diet, physical activity, and, in selected cases, weight-loss injections, which reduced the severity of apnea in recent studies.
Frequently asked questions
Can someone with apnea have a heart attack?
The risk is higher, yes. Untreated apnea overloads the heart night after night, favors high blood pressure and arrhythmias, and, in severe cases, long-term studies showed about three times more cardiovascular events in those who did not treat it. That is why apnea should be investigated and treated early, together with the other heart risk factors.
Does apnea cause stroke?
Sleep apnea is an independent risk factor for stroke. A classic study in the New England Journal of Medicine showed about twice the risk of stroke or death in people with obstructive apnea. The repeated drops in oxygen and the pressure spikes during the night explain much of that risk.
What are the consequences of sleep apnea?
Untreated, apnea is associated with high blood pressure, arrhythmias such as atrial fibrillation, heart attack, stroke, insulin resistance and diabetes, decline in memory and concentration, sleepiness with a risk of accidents, irritability, depression, and reduced libido. Most of these consequences improve or stop progressing once apnea is treated.
What is a person with sleep apnea like?
The typical picture is of someone who sleeps but does not rest: they wake up tired, have a morning headache, feel sleepy during the day, become irritable easily, and notice worse memory and concentration. At night, they snore loudly and have breathing pauses that tend to frighten whoever sleeps beside them. Many only realize how poorly they were living after they start treatment.
What is the medication for sleep apnea?
There is no drug that keeps the airway open during sleep. The recent development is weight-loss injections: in people with apnea linked to obesity, tirzepatide reduced the severity of apnea in a large study, through weight loss. They act on the cause in selected cases, with a medical prescription, and do not replace assessment of the airway or the other treatments.
Can someone with sleep apnea take sleeping pills?
With great caution, and never on your own. Several sleep aids and sedatives relax the throat muscles even more and can increase the number and duration of breathing pauses. If you snore or suspect apnea and sleep poorly, the way forward is to investigate and treat the apnea first. When a medication is necessary, it should be chosen by a physician who knows your sleep study.
The first step is to investigate
If you snore every night, wake up tired, or have caught a family member pausing their breathing, do not wait for the problem to charge a higher price. Sleep apnea has effective treatment for every degree, and a cure in specific situations. The sooner you find where the obstruction is, the greater the chances of a complete result.
Dr. José Eduardo Marcondes is a PHYSICIAN and otolaryngologist (ENT) (CRM SP 107711 | RQE 43840), working in nasal surgery and in the treatment of snoring and sleep apnea, seeing patients in Morumbi and Itaim (São Paulo) and in Alphaville (Barueri). If it makes sense for you, book a consultation so we can investigate your sleep and talk about the best path for your case.
References
- Tufik S, Santos-Silva R, Taddei JA, Bittencourt LR. Obstructive sleep apnea syndrome in the São Paulo Epidemiologic Sleep Study. Sleep Medicine. 2010;11(5):441-446. doi:10.1016/j.sleep.2009.10.005.
- Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365(9464):1046-1053. doi:10.1016/S0140-6736(05)71141-7.
- Yaggi HK, Concato J, Kernan WN, Lichtman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a risk factor for stroke and death. New England Journal of Medicine. 2005;353(19):2034-2041. doi:10.1056/NEJMoa043104.
- Malhotra A, Grunstein RR, Fietze I, et al. Tirzepatide for the treatment of obstructive sleep apnea and obesity (SURMOUNT-OSA). New England Journal of Medicine. 2024;391(13):1193-1205. doi:10.1056/NEJMoa2404881.
- McEvoy RD, Antic NA, Heeley E, et al. CPAP for prevention of cardiovascular events in obstructive sleep apnea (SAVE). New England Journal of Medicine. 2016;375(10):919-931. doi:10.1056/NEJMoa1606599.
This content is informational and does not replace a medical consultation.
Read also:
About the author
Dr. José Eduardo Marcondes
Otolaryngologist (ENT) · CRM-SP 107.711 · RQE 43.840
Trained and completed his residency at Escola Paulista de Medicina (UNIFESP), with more than two decades of experience. A pioneer in the use of robotic surgery (TORS) for sleep apnea. Member of the clinical staff at Hospital Albert Einstein, Vila Nova Star and São Luiz. Member of ABORL-CCF.
Learn about his full career → · Schedule an appointment on WhatsApp