Obstructive sleep apnea is usually pictured as a problem of the “man who snores loudly.” That image holds some truth, but it tells only half the story. Apnea also affects women, and it often goes unnoticed precisely because it shows up differently from what people expect. Understanding these differences helps both those who share a bed with a snorer and those who feel tired and sleep poorly without knowing why.
This article about sleep apnea in men and women is educational: it shows how the condition behaves in each sex, why it is underdiagnosed in women, and what changes (and what does not) when it comes to investigating and treating it.

What obstructive sleep apnea is
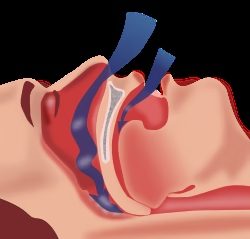
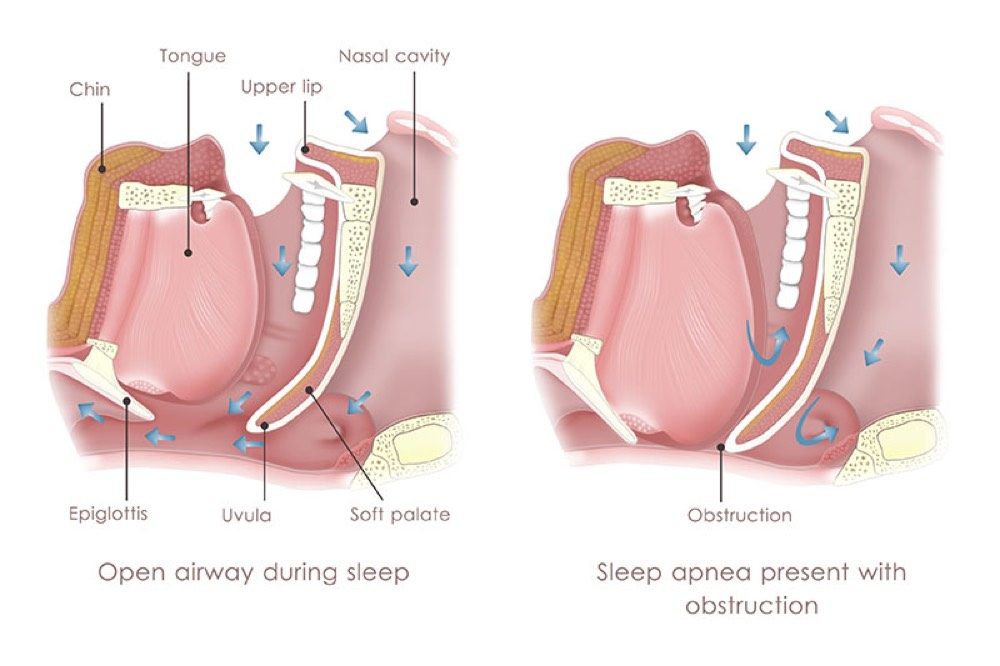
During sleep, the muscles of the throat relax. In people with a narrower airway or more lax tissues, this relaxation can briefly close off the passage of air, interrupting breathing for a few seconds, several times a night. Each pause makes the brain react with a micro-arousal in order to start breathing again. Sleep becomes fragmented, the body does not truly rest, and blood oxygen fluctuates throughout the night.
This is obstructive sleep apnea. It affects men and women alike, but the way it appears, is noticed, and is even diagnosed changes with sex.
Prevalence and epidemiology: more common in men, but not rare in women
Apnea is, in fact, more frequent in men. One of the landmark population studies, the Wisconsin Sleep Cohort, found sleep-disordered breathing (defined as an apnea-hypopnea index of 5 or more per hour of sleep) in about 24% of middle-aged men and 9% of middle-aged women. The classic ratio described is roughly 2 to 3 men for every woman in the general population.
But that figure hides a trap. In clinics and sleep laboratories, for a long time the ratio seemed even higher (it was sometimes described as 8 or 10 men for every woman), not because women are so much less affected, but because they were referred for investigation far less often. In other words, part of the difference between the sexes is not biological, it is diagnostic.
There is also a factor that changes everything over the course of a woman’s life: menopause. Before it, a woman’s risk is lower. Afterward, prevalence rises markedly and approaches that seen in men. Apnea, then, is not a “man’s disease,” but a condition that is distributed differently between the sexes and over time.
Causes: why men tend to have more
The differences begin with anatomy and physiology.
- Fat distribution. Men tend to accumulate fat around the neck and abdomen (the android pattern), which increases pressure on the airway and the effort of breathing while lying down.
- Airway shape and length. The male airway tends to be longer and more prone to collapse during sleep.
- Female hormonal protection. Before menopause, female hormones (especially progesterone and estrogen) help maintain respiratory drive and the tone of the muscles that support the throat. This acts as partial protection. With the hormonal decline of menopause, this protection lessens and risk increases.
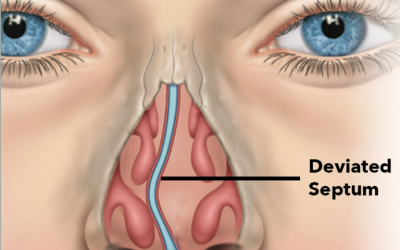
In women, other triggers also come into play: weight gain, polycystic ovary syndrome, and pregnancy itself, a period in which hormonal and anatomical changes can favor the onset or worsening of apnea. In both sexes, nasal obstruction (from a deviated septum, enlarged turbinates, or rhinitis) and excess weight often contribute to the problem.
Symptoms: the same condition, two different portraits
Here is perhaps the most important difference of sleep apnea in men and women in practice.
In men, apnea usually presents in the “classic” portrait, the one most people recognize:
- loud, persistent snoring;
- pauses in breathing noticed by the person sleeping beside them;
- excessive daytime sleepiness (dozing off in meetings, in traffic, while reading).
In women, symptoms tend to be less typical and, for that reason, more easily confused with other conditions:
- tiredness and lack of energy (more than “sleepiness” as such);
- insomnia or unrefreshing sleep;
- headache on waking;
- mood changes, such as anxiety and depressive symptoms;
- difficulty with concentration and memory.
Snoring does occur in women, but it is usually reported as milder, and breathing pauses are noticed less often. As a result, the complaint that leads to diagnosis frequently never surfaces.

The way symptoms are expressed also differs
It is not only the body that behaves differently: so does the way people describe what they feel. Many women do not report snoring spontaneously, whether because they sleep alone and no one observes them, or because of a social embarrassment still attached to snoring in women. And when they describe feeling unwell, they tend to use words like “tiredness,” “exhaustion,” or “stress,” rather than “daytime sleepiness.”
Men, on the other hand, often come to the office prompted by the complaint of whoever shares their bed: it is the loud snoring and the breathing pauses that trigger the search for help. This difference in how symptoms are reported means that apnea in men is “seen” more easily, while apnea in women stays silent for longer.
Effects on life and health
Untreated apnea goes well beyond poor sleep. In both sexes, it is associated with a higher risk of hypertension, arrhythmias, cardiovascular disease, metabolic changes, and worse quality of life.
In women, some aspects deserve special attention. Mood and fatigue symptoms tend to weigh heavily on daily life and on the sense of well-being. And during pregnancy, apnea is associated with a higher risk of complications such as gestational hypertension, preeclampsia, and gestational diabetes, which reinforces the importance of investigating sleep during this period as well.
In men, earlier diagnosis is an advantage, but daytime sleepiness carries concrete risks, such as traffic and workplace accidents, along with an impact on performance and relationships.
How each sex tends to cope with the condition
Because they are referred less and later, many women spend years with symptoms attributed to depression, hypothyroidism, anemia, fibromyalgia, or “menopause things” before apnea is even considered. This delay in diagnosis is one of the most important points to correct.
In men, the path to diagnosis tends to be shorter, especially when a partner notices the snoring and the pauses. Once diagnosed, men and women may face different strengths and difficulties in sticking with treatment, which is why close follow-up, adjusting whatever is needed, makes a difference to the outcome.
The practical message is simple: chronic tiredness, unrefreshing sleep, morning headache, and mood changes warrant a sleep evaluation, even without the thunderous snoring of the classic portrait.
Diagnosis: the same test, with a close eye on the differences
Diagnosis does not use a different test according to sex, but it does require attention so that apnea in women is not missed. The evaluation usually includes:
- a detailed conversation about sleep, symptoms, and habits;
- examination of the airway, often with nasal endoscopy, to check whether a nasal component is contributing;
- when indicated, polysomnography (the “sleep study”), which confirms the diagnosis and grades its severity.
One extra caution is worth noting: in women, apnea tends to concentrate in certain sleep stages (such as REM sleep) and in certain positions, and the index of events per hour may be lower even when symptoms are significant. For that reason, the number from the test alone must always be interpreted together with the person’s clinical picture.

Treatment of sleep apnea in men and women: the same principles, individually tailored
Treatment options are, on the whole, the same for men and women, and the choice depends on severity, anatomy, and each person’s lifestyle:
- CPAP: continuous positive airway pressure remains the most established treatment for moderate to severe apnea in both sexes.
- Oral appliance and positional therapy: useful in selected cases, especially when apnea is milder, positional, or concentrated in REM sleep, a pattern common in women.
- Treating the nose: when nasal obstruction is part of the problem, septoplasty and turbinoplasty can improve breathing and even help with CPAP adherence.
- Laser: for snoring and mild to moderate apnea, the Fotona laser (NightLase protocol) can be a non-surgical alternative. It involves 3 to 4 in-office sessions, with good results in selected cases.
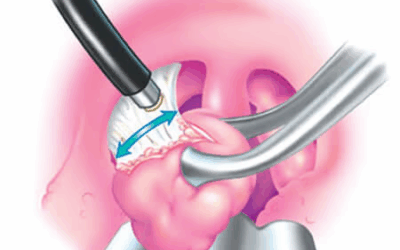
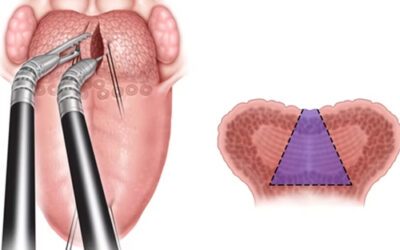
- Surgery: in some cases, surgery, such as septoplasty, transoral robotic pharyngoplasty (TORS), or barbed reposition pharyngoplasty, can be a treatment option in patients with favorable anatomical features.
- Lifestyle changes: weight control and attention to alcohol at night and to sleep are also part of treatment, whatever the sex.
In women, it is also worth considering the stage of life (menopause and pregnancy, for example) when deciding on the best strategy. In every case, the goal is the same: to treat the cause of the obstruction, not merely to silence the snoring.
Frequently asked questions
Is sleep apnea only a man’s problem?
No. Apnea is more frequent in men, but it also occurs in women, especially after menopause. Much of the observed difference comes from the fact that the condition is investigated less often in women, not simply from women being affected less.
Why is apnea harder to diagnose in women?
Because the symptoms tend to be less typical: tiredness, insomnia, headache on waking, and mood changes, rather than loud snoring with pauses. These signs are easily confused with depression, stress, or menopause symptoms, which delays diagnosis.
Does snoring only a little mean I don’t have apnea?
Not necessarily. Snoring can be mild or barely noticed, especially in women, and apnea may still be present. If there is persistent tiredness, unrefreshing sleep, or sleepiness, it is worth investigating.
Does menopause increase the risk of apnea?
Yes. As female hormones decline, the partial protection against apnea lessens, and prevalence in women rises, approaching that seen in men.
Is apnea in pregnancy a cause for concern?
It can be. Apnea during pregnancy is associated with a higher risk of gestational hypertension, preeclampsia, and gestational diabetes. Sleep symptoms in pregnancy warrant evaluation.
Is the treatment different for men and women?
The principles are the same (CPAP, treating the nose, an oral appliance, lifestyle changes, laser, or surgery in selected cases). What changes is the individual tailoring, taking into account anatomy, severity, sleep pattern, and each person’s stage of life.
It’s worth discussing your case
If you (or someone close to you) has tiredness that won’t go away, unrefreshing sleep, snoring, or breathing pauses, the first step is an evaluation that gets to the origin of the problem. Sleep apnea is treatable, and recognizing that sleep apnea in men and women shows up differently is part of reaching the right diagnosis.
Dr. José Eduardo Marcondes is a PHYSICIAN and otolaryngologist (ENT) (CRM SP 107711 | RQE 43840), working in nasal surgery and in the treatment of snoring and sleep apnea, seeing patients in Morumbi and Itaim (São Paulo) and in Alphaville (Barueri). If it makes sense for you, book a consultation so we can discuss your case.
References
- Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. New England Journal of Medicine. 1993;328(17):1230-1235. doi:10.1056/NEJM199304293281704.
- Bonsignore MR, Saaresranta T, Riha RL. Sex differences in obstructive sleep apnoea. European Respiratory Review. 2019;28(154):190030. doi:10.1183/16000617.0030-2019.
- Lin CM, Davidson TM, Ancoli-Israel S. Gender differences in obstructive sleep apnea and treatment implications. Sleep Medicine Reviews. 2008;12(6):481-496. doi:10.1016/j.smrv.2007.11.003.
This content is informational and does not replace a medical consultation.